
Survivors

Find practical advice, emotional support, and resources to help you or your loved one cope with the challenges of living with lung cancer.


July 6, 2026

Laura lives in Camden, South Carolina, where she loves horseback riding, playing Mahjong, and is opening her very own Mahjong studio. She is a Veteran who receives care through the Veterans Administration (VA) and is an active advocate for lung cancer awareness.
Laura never expected lung cancer to be part of her story. At 38, she was doing everything she was supposed to do. She was keeping up with annual appointments through the VA, staying active, and paying attention to her health. Lung cancer wasn’t even on her radar.
But looking back, there were signs. She had a lingering cough that began the previous spring, fatigue that she chalked up to stress from work and life, and congestion that allergy medications never seemed to touch. Occasionally, she even coughed up blood. But like many people, especially younger people, she never imagined it could mean lung cancer.
“I was so focused on all the other cancers,” Laura said. “My mom died of colon cancer, so I started getting colonoscopies in my twenties. I kept up with everything they tell you to be aware of related to women’s health. But lung cancer was nowhere on my radar.”
During a routine visit at the VA in April 2023, Laura mentioned the cough to her doctor, along with wrist pain, exhaustion, and a handful of other symptoms that had slowly become part of everyday life. Because Veterans are diagnosed with lung cancer at higher rates than the general population, her care team ordered a chest X-ray right away.
The chest X-ray appeared to show a small 6-millimeter nodule in her right lung. It was small enough that her care team reassured her it was common in service members. They'd just monitor it with a CT scan to make sure it wasn't growing.
Then the CT results came back. The nodule wasn't 6 millimeters. It was almost 6 centimeters.
Her doctor called her that afternoon. She told Laura she was sorry and that she was going to schedule her with an oncologist right away. Laura didn't even know what to say.
"I'm sorry, ‘oncologist?’ What do you mean? Why do I need an oncologist? Could it be anything else?" she asked.
"Based on the size of [the nodule]," the doctor told her, "No. It's going to be cancer."
The importance of biomarker testing
A few days later, Laura underwent a biopsy through the VA’s partnership with the Medical University of South Carolina (MUSC). Her pulmonologist immediately emphasized the importance of comprehensive biomarker testing before starting treatment. It’s a step that Laura now knows was critical.
“They said, ‘We’re going to get a lot of tissue, send it for genetic testing, and wait for those results before deciding on treatment,’” she said. “I was lucky. This is how everybody should be treated.”
The results confirmed that Laura had stage 4 (IV) ALK-positive lung cancer, a form of non-small cell lung cancer (NSCLC) driven by an ALK biomarker. Although hearing the words “stage 4” was devastating, learning she had a biomarker also meant she had highly targeted treatment options available.
At first, Laura started treatment with alectinib, an ALK-targeted therapy. But while the medication effectively treated her cancer, the side effects became difficult to manage.
Eventually, after struggling with side effects and elevated liver enzymes, Laura transitioned to lorlatinib, another ALK-targeted therapy she says has allowed her to regain much of her quality of life.
“I have energy again,” she said. “It’s so much better.”
Learning to live with uncertainty

Still, adjusting to life with metastatic lung cancer has been about far more than finding the right medication. Laura describes the emotional aftermath of diagnosis as one of the hardest parts of her experience.
“The diagnosis is world-upending,” she said. “First, you think you’re going to die. Then, actually, no. Maybe you’re not going to die right away. And, OK, you’re excited to be doing so well, but now you have to figure out how to live this entirely new way.”
Over time, Laura has learned that coping doesn’t always mean fixing everything. In fact, some of her biggest lessons have come from letting go of the illusion of control.
“I went a little crazy trying to control everything at first,” she said. “I changed my diet, exercised constantly, and stopped drinking alcohol overnight. I just wanted to do something.”
“Over time, I had to learn to let go a little, and that I don’t need to solve every bad feeling,” she said. “I control what I can control and let the bad days come when they come. It doesn’t mean it’s forever.”
That shift in perspective has helped Laura rebuild a life that still feels joyful and meaningful. After her diagnosis, she moved to Camden, South Carolina, where she now spends time horseback riding, playing mahjong, and preparing to open a mahjong studio, a project she enthusiastically describes as her latest obsession.
“When I’m into something, I’m serious about it,” she laughed. “It’s been good to channel that energy from cancer to something more fun.”
Finding community and hope
Laura has also become involved in advocacy through GO2 for Lung Cancer and the ALK Positive community. Attending advocacy events and scientific summits has transformed the way she thinks about the future.
“Every year at the ALK Summit, researchers and doctors show us what they’re working on,” she said. “You realize there are absolutely brilliant people out there who care deeply about helping us live longer.”
Sharing her story on Capitol Hill during GO2’s Voices Summit has also shown her how much education is still needed around lung cancer.
“I realized legislators and staffers often don’t know anything about lung cancer,” she said. “Sharing my story was an opportunity to teach them about the disease and what is needed to better treat it.”
Today, Laura hopes her story helps challenge outdated assumptions about who gets lung cancer and what life after diagnosis can look like, especially for younger people, Veterans, and people living with biomarker-driven disease.
Her biggest advice for someone newly diagnosed?
“Take your time,” she said. “You don’t have to figure everything out right now.”
She also strongly encourages others to find community.
“The biggest help for me was joining a supportive group and talking to people going through the same thing,” Laura said. “You realize you’re not alone, and that’s priceless.”
“There’s so much more coming”
Three years after her diagnosis, Laura knows life still includes uncertainty, grief, and hard days. But it also includes hope, connection, and plans for the future.
“It’s so empowering to see all the advances happening in research,” she said, “I really believe there’s so much more coming.”
A lung cancer diagnosis can bring a lot of questions, emotions, and uncertainty. GO2 for Lung Cancer's free HelpLine connects you with trained specialists who can provide support, answer questions, and help you find resources along the way. Whether you're newly diagnosed, in treatment, or navigating survivorship, you don't have to face it alone.
Call us at 1-800-298-2436 or email support@go2.org to learn more.
June 5, 2026
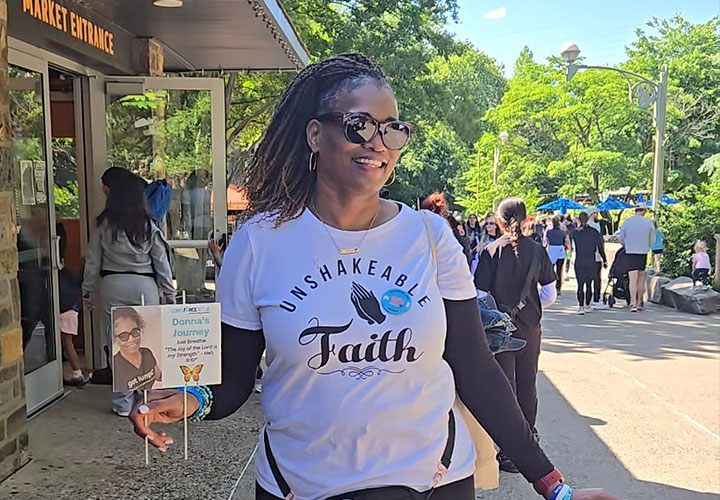
Donna Thompson is a 3-time survivor of early-stage, non-small cell lung cancer, thriving more than a decade since her first diagnosis. After 2 surgeries to remove portions of her right lung, she carries forward an experience that deepens her commitment to lung cancer awareness, mental health advocacy, and building supportive communities. Donna shares her story to inspire hope, reduce stigma, and elevate survivor voices. Her advocacy spans education, outreach, and research collaboration within the lung cancer community. She speaks at wellness and community events, using her experience to empower others navigating illness and recovery. Professionally, Donna is the director of Human Resources and a SHRM Certified HR leader, known for leading with empathy and practical insight, and supporting people through complex workplace challenges. She finds strength - literally and emotionally - through faith, fitness training, and time in nature. For her, movement is medicine, and advocacy is a calling rooted in compassion and resilience.
Donna remembers the exact moment everything changed. It was September 2015, and she went to the emergency room for something else entirely. Her blood sugar was dangerously high, and she wasn’t feeling right. They ran tests, monitored her, and sent her home. The next day, the ER doctor called her and said the radiologist saw a mass in her lung and that she should have it checked out right away.
At 45 years old, and having no smoking history, lung cancer wasn’t on her radar. It wasn’t on anyone else’s either.
“Everyone I talked to was like, ‘You’re too young. You’ve never smoked. This is probably not lung cancer.’”
But within 5 weeks, after scans, a biopsy, and what she still calls “the longest 5 weeks of my life,” Donna had her answer. It was lung cancer after all.
"The best possible situation”
Looking back, Donna sees the moments that led to her lung cancer diagnosis a little differently.
“I always say that was God getting my attention, whispering to me in the quiet, still moments," she said.
The tumor was stage 2 (II) and operable. In many ways, it was the best-case scenario for a diagnosis no one expected. Her surgical team moved quickly.
“She told me, ‘This is the best possible situation. It’s in a good location. We can take it out.’”
By the end of November, just 2 months after that ER visit, Donna had surgery, and for a moment, it felt like the worst might already be behind her.
When the plan changes
Initially, Donna was told she wouldn’t need chemotherapy. The surgery had been successful, her margins were clean, and everything pointed in the right direction.
Then the pathology report came back. It showed that her tumor was more complex than expected. It was an unusual form of adenocarcinoma that didn’t behave in typical ways. Her case was sent to multiple cancer centers, and the recommendation shifted.
“I remember my surgeon calling me herself,” Donna said. “She said, ‘I told you one thing, and now it’s changing, and I need to explain that to you.’”
A second opinion confirmed it: chemotherapy was recommended. Donna agreed, but her body had other plans.
When treatment becomes the crisis
“Every time I got chemo, I ended up in the ER,” she said. “Something was always going wrong.”
After just two treatments, it was clear that this wasn’t sustainable. Her oncologist made the call.
“He said, ‘Your body can’t handle this. We’re done.’”
It was a moment that carried both relief and uncertainty. The treatment meant to protect her was, instead, putting her in danger. And so, once again, Donna adjusted.
“I didn’t survive to be basic.”
In the months that followed, Donna made a decision that would shape everything that came next.
“I didn’t survive to be basic,” she said.
Instead, she poured herself into her health and started working with a trainer, changing her diet, and reclaiming a sense of control over her body.
“I got into the best shape of my life,” she said. “I came off medications. My A1C went back to normal. Everything changed.”
But the transformation wasn’t just physical. It was also about identity.
“The cancer gave me more than it took from me,” she said. “I learned who I am, how strong I can be, and what I really need in the world. I learned what and who are important to me. It put such a clear focus on what I want for my life.”
Finding community and belonging
Still, parts of the experience felt isolating.
“I kept meeting people, and they were all stage 4 (IV),” she said. “I felt like, am I even supposed to be here?”
She was grateful for her outcome, but that gratitude came with a quiet tension.
“I didn’t want to take up space in their groups,” she said. “But I still needed support too.”
And there was something else. “I didn’t see anyone who looked like me.”
It wasn’t until years later, through social media connections, introductions, and small group conversations, that Donna found what she had been missing: a close-knit circle of Black women who truly understood her experience.
“We started meeting regularly, talking, and supporting each other,” she said. “There’s something about being with people who understand you completely without you having to explain that changes everything. They know what they did for me, and what we do for one another. Finally, I had community.”

A second diagnosis, and a different reality
For nearly 7 years, Donna focused on moving forward, rebuilding, and holding onto the belief that she had come through something and grown because of it.
Then, in 2022, everything shifted again. This time, it wasn’t a symptom that sent her back to treatment. It was a scan.
“My scans went from showing nothing to showing a tumor the same size as my first diagnosis,” she said. “I was just so shocked because I wasn’t expecting anything.”
As Donna began to piece together what had happened, the story became even more complicated. The tumor hadn’t appeared overnight. When her new care team reviewed her prior scans, they discovered that the growth had been visible as far back as 2018, but it had been missed.
The radiologist who originally read the scan had not flagged it, and even more concerning, it became clear that her oncologist had never reviewed the images directly.
“That was the moment for me,” Donna said. “I realized no one had really been looking out for me the way they should have. I felt like a number, and I’m a relationship person. This matters to me.”
It was a turning point, not just medically, but emotionally. What initially felt like a sudden recurrence became something harder to process. It was a missed opportunity for earlier intervention.
Another treatment crisis
This time, Donna’s treatment plan included a targeted therapy designed specifically for EGFR-positive lung cancer that would allow her to take a lower dose of chemo, which they hoped she would tolerate better. It felt like progress and a better path.
But after a second surgery, adjuvant chemo, and introducing the new treatment, her body began to struggle again in a different and even more frightening way, this time in response to the targeted therapy.
After multiple attempts to adjust the dosage, the new medicine ultimately led to kidney failure, a serious complication that forced yet another shift in her care and another redefinition of what “moving forward” would look like.
It was also the moment that changed how Donna understood her own story.
“I used to say that cancer gave me more than it took from me,” she said. “And I believed that until my kidneys failed. Recovering from that took nearly all I had. I’m still trying to fully move on from how traumatic that year was.”
“I also have to remind myself how remarkable it was that I overcame this,” she said. “My nephrologist said my recovery was miraculous, and it does feel like a total miracle now.”
Living in the in-between
Today, Donna is once again in a place that many people with lung cancer know all too well: waiting.
In July 2025, after recovering from kidney failure, her care team radiated 2 new spots. They chose radiation because it was the gentlest option for her. Recent scans have shown new nodules that Donna and her care team are just watching, for now.
“They’re watching them and trying to decide what to do next,” she said. “And with my treatment history, not every option feels like a good one.”
It’s not a crisis. But it’s not clarity, either, and Donna finds herself struggling with living in this place of uncertainty.
“I like to have a plan, and I like to know what we’re going to do. I’m finding it very hard for me to just wait and see.”
Still choosing more
Through her diagnosis, treatment, recurrence, and all the unexpected turns in between, Donna has held onto a simple mindset:
“I didn’t survive to be basic.”
It’s a phrase that stuck with her early on and has continued to shape how she moves through each new chapter. And for Donna, that means continuing to choose a full life, even in the unknown.
If you or someone you love has been diagnosed with lung cancer, know that you're not alone. Our HelpLine provides free, one-on-one support to people impacted by the disease. Call 1-800-298-2436 or email support@go2.org to connect. Our team is available Monday-Friday from 9 a.m.-5 p.m. ET/6 a.m.-2 p.m. PT.

May 6, 2026

Michelle Bos-Lun is a third term state representative in the Vermont General Assembly. She lives in Westminster with her husband. She has 3 adult children and 2 grandchildren. Michelle is an enthusiastic vegan cook and baker, a mushroom forager, a hiker, and an advocate for lung cancer.
When Michelle returned home from a trip to Nepal last year, she soon found herself unable to get out of bed. At first, she thought she had jet lag, but when her symptoms worsened, she ended up in the hospital.
What followed was a whirlwind of tests and uncertainty that led to a diagnosis she hadn’t expected: scrub typhus, a rare and potentially life-threatening infection she had contracted while traveling.
But the story didn’t end there. In the process of trying to understand why she was so sick, doctors ordered a chest X-ray and saw something there that they couldn’t explain.
Three weeks and even more tests later, Michelle received a second surprising diagnosis: lung cancer.
A diagnosis she never expected
Like so many others, lung cancer wasn’t something Michelle imagined would happen to her until it did.
“Before my diagnosis, I knew of one person who had lung cancer without a smoking history,” she said. “So, while I knew it was possible, it didn’t seem at all likely. But lots of people aren’t good candidates for lung cancer, and yet it still finds us.”
Still, even in the face of a stage 3B (IIIB) diagnosis, her reaction was not what many might expect.
“I’m pretty pragmatic about things,” she said. “When something comes up, I want to learn all about it and figure out what I can do to have the best results with a situation that isn’t ideal.”
That instinct to learn, adapt, and move forward has shaped everything that’s followed

“I won the lottery”
After her initial diagnosis, Michelle entered a waiting period, one filled with a lot of questions, but few clear answers. Her oncologist couldn’t yet tell her what kind of lung cancer she had or how it would be treated. The outlook he shared at that point was sobering.
But there was one 1 possibility that offered hope, and that was a genetic mutation.
Her doctor told her, “If you have a mutation, there are some really good targeted therapies.”
Two weeks later, the call came. Michelle had ALK-positive lung cancer.
“He told me I won the lottery,” she said. “I had the best one with the best treatment.”
Within days of starting the targeted therapy, Lorbrena (loralatinib), her persistent cough, which was her only noticeable symptom, had disappeared. A few months later, her first scan showed her cancer had been reduced by nearly 50%.
“My doctor actually said, ‘This is even better than I would have expected,’” Michelle said.
A whole-person approach
From the beginning, Michelle approached her diagnosis the same way she has approached much of her life by integrating different perspectives, experiences, and tools. Having spent part of her adolescence in Taiwan, and as a long-practicing Buddhist, she was already comfortable holding multiple ways of thinking at once.
“My life has been a mixture of East and West since I was 12,” she said. “So, when I got cancer, it made sense to include a variety of different resources and approaches.”
Her treatment plan reflects that. Alongside her targeted therapy, Michelle has built a daily routine that supports her body in other ways:
- Tai Chi twice a day to improve circulation and manage neuropathy
- Walking several miles each day
- Bi-weekly acupuncture
- Regular lymphatic massage
- A nutrient-dense, plant-based diet including daily kale smoothies, large salads, and roasted vegetables with whole grains
“I feel as healthy as I’ve ever been. Except I have cancer,” she said.
It’s a paradox she doesn’t shy away from. And it’s one she’s actively working to sustain.
“The lorlatinib gets credit for 75% of my healing, and my kale smoothies get the other 25%,” she joked.
Choosing hope—on purpose
Michelle is quick to acknowledge that everyone responds to a diagnosis differently. But for her, hope is not something she has to force; it’s something she naturally gravitates toward.
“I think you can choose to look at the hardest parts, or you can look at the possible good outcomes,” she said. “For me, it’s more satisfying to look at the positive. I try to find the best-case scenarios and aim for those.”
Even before her diagnosis was confirmed, she made a conscious choice not to dwell in pessimism.
“Before my lung biopsy, I thought, I don’t think it’s very likely that this is lung cancer, so I’m not going to worry about it,” she said. “And then when it turned out to be cancer, I said, ‘Okay, so when can we figure out how to treat this?’ I could have spent that time scared, but being scared wouldn’t have changed the outcome, only how I experienced the time leading up to it. That’s sort of how I approach everything.”
Finding community and perspective
Like many people diagnosed with a biomarker-driven form of lung cancer, Michelle quickly found community among others living with ALK-positive disease.
“I feel like I’ve been welcomed into this club that none of us wanted to join,” she said. “But since we’re here, we’re there for each other.”
Through that community, she found not only information, but perspective, including examples of people living 10, 15, even 20 years after diagnosis. Their stories helped her understand the full range of what’s possible and where she might fit within it.
“Somebody would say, ‘my husband is 21 years out’, and I thought, what? We can live 21 years with this? Knowing that some people can live quite a long time made me feel like, okay, then I can make it too,” she said.

Not waiting anymore
If there is 1 theme that runs through Michelle’s story, it’s this: don’t wait.
After her diagnosis, she began thinking about the people she hadn’t seen in years and the friendships that had drifted with time and distance. She immediately set out to rectify that. Her first trip was to reconnect with a close friend she hadn’t seen in decades.
“I just thought, I don’t want to wait,” she said. “Why did I already wait 30 years? I’m not doing that again.”
Now, her “bucket list” isn’t about places; it’s about people – reunions, visits, and time spent together.
“I hope I’m going to be around for a long time,” she said. “But in case I’m not, I don’t want to wait to spend time with the people who matter most to me. I want to see them now.”
Turning experience into action
As a state legislator in Vermont, Michelle already had a platform. After her diagnosis, she chose to use it in a new way. From the very beginning, she has spoken publicly about her experiences, using them as an opportunity to raise awareness about lung cancer, and especially the importance of early detection.
“I thought, maybe I can help somebody else,” she said. “If I can help educate someone, then go ahead, use my story.”
After her story appeared on the front page of her local paper, she learned that at least two people went to their doctors to ask for chest X-rays. For Michelle, that was enough.
“That’s the whole point,” she said.
She is also working to connect her personal experience with broader public health efforts, including initiatives that emphasize nutrition as a core component of care.
“When people eat healthy food, it helps keep them healthy,” she said. “I’m a living example of that.”
Moving forward
Less than a year into her diagnosis, Michelle’s life looks both familiar and entirely new. She is still working, still advocating, and still showing up for her family.
But she is also living with a deeper sense of urgency and intention.
“When you get lemons, make lemonade,” she said. “Well, I’m making some lemonade.”
Only in Michelle’s case, it’s likely organic, and paired with a kale smoothie.
A lung cancer diagnosis can bring a lot of questions, emotions, and uncertainty. GO2 for Lung Cancer’s free HelpLine connects you with trained specialists who can provide support, answer questions, and help you find resources along the way. Whether you’re newly diagnosed, in treatment, or navigating survivorship, you don’t have to face it alone.
Call us at 1-800-298-2436 or email support@go2.org to learn more.

May 5, 2026

For Amita Jain, MD, lung cancer is not just a diagnosis. It’s a lived experience that has shaped her life across multiple roles as a physician, a patient, a daughter, a caregiver, and an advocate.
Her family’s lung cancer story spans generations. In July 2018, her mother, Usha Jain, a retired UC Berkeley professor, was diagnosed with stage 4 (IV) non-small cell lung cancer (NSCLC) despite having no smoking history. Just 6 months later, Amita herself would receive the same diagnosis.
While both women faced advanced disease, their treatment paths diverged. Usha underwent chemotherapy and immunotherapy for nearly 2 years before stopping treatment and transitioning to routine scans. That period (often described clinically as “watch and wait”) felt anything but passive to her family.
“It was hard to feel as though we were ‘doing nothing,’” Amita recalls.
Turning to navigation for answers
As both a physician and a caregiver, Amita understood medicine, but even she found the complexity of lung cancer care overwhelming.
Navigating next steps after treatment, understanding emerging options, and keeping up with rapidly evolving research can feel like a full-time job, especially for families already carrying the emotional weight of a diagnosis.
So, Amita reached out to GO2's LungMATCH navigation program.
“I called the navigators and furnished my mom’s tumor’s genetic profile,” she says. “They reached out a day later with information on some trials for which she might qualify.”
Although her mother ultimately chose not to pursue clinical trials, the impact of that interaction was profound.
“While we did not take action on the options that the navigator provided, the information was empowering,” Amita explains. “It really helped us understand the ‘lay of the land’ in her particular situation.”
Bridging the gap between information and understanding
Even for someone with medical training, the experience revealed an important truth. Access to information is not the same as understanding it.
“Navigating is complex and scary, and getting all the information is difficult if you are not an oncologist,” Amita says. “The navigator that I spoke with was both professional and prompt. That information made me feel as though we understood our options—and that was extremely reassuring.”
For patients and families, that reassurance can be transformative.
A lung cancer diagnosis often brings not only fear, but also a sense of powerlessness. Decisions feel urgent; stakes are high, and the volume of information can be paralyzing.
“The navigator can serve as a bridge to knowledge,” Amita says. “Knowledge is power. Having a diagnosis of lung cancer can be shocking, but more importantly you do feel a bit powerless and overwhelmed. The navigators serve as a resource and lifeline.”
The invisible work of navigation
What many patients don’t see is the depth of work happening behind the scenes.
Navigators are constantly reviewing evolving research, identifying clinical trials, interpreting biomarker data, and translating complex medical information into something patients can actually use to discuss with their care teams.
“Keeping up on the information is a full-time job that most of us are not trained to do,” Amita says.
That expertise becomes especially critical at moments of uncertainty, like when treatment ends, and the path forward is unclear.
In those moments, navigation doesn’t just guide decisions; it restores a sense of control.
Strengthening navigation for the future
Stories like Amita’s mother’s underscore the critical role navigators play, not just in coordinating care, but in empowering patients and families with clarity, confidence, and connection.
To support and strengthen this role, GO2 for Lung Cancer partnered with leading experts to develop a comprehensive resource for those on the front lines of patient care.
The Lung Cancer Navigator: A Guide for Nurses and Allied Health Professionals textbook is designed to equip health professionals with the knowledge and tools they need to guide patients through every step of the lung cancer experience, from diagnosis to survivorship.
By investing in navigator education, we can ensure that more patients and families experience what Amita describes so clearly: the shift from feeling overwhelmed and uncertain to being informed and empowered.

March 10, 2026

Brenda S. didn’t expect anything unusual from her visit to her primary care physician. It was the kind of routine appointment she had done many times before. It was a standard check-in, familiar questions, nothing out of the ordinary. Brenda had lived with multiple sclerosis (MS) for years and understood what it meant to manage a chronic illness, but aside from that, she considered herself healthy. Lung cancer was not on her radar.
And yet, that appointment marked the beginning of an experience that would change her life.
“You better get another opinion.”
Brenda’s experience with lung cancer stands out because it didn’t follow the path so many others know too well.
“A lot of times people are diagnosed at a pretty late stage,” she explained. “I was one of the lucky ones to get diagnosed early.”
That early diagnosis, however, didn’t come easily or immediately, and it didn’t come without persistence.
During that initial visit, something caught her doctor’s attention. Tests followed, and eventually, her doctor discovered a nodule. Brenda was told that it was benign. On the surface, that should have been the end of the story. Relief is the word most people would expect to describe that moment.
But relief wasn’t the whole truth.
“I remember just saying, please, please don’t let it be cancer,” Brenda recalled. And when she heard the word benign, she wanted to believe it completely. Yet underneath the reassurance, there was a feeling she couldn’t shake. “Deep inside, it was nagging,” she said. “It was like… I don’t know, sister, you’d better get another opinion.”
Brenda tried to move forward. Life went on. But that quiet inner voice didn’t disappear.
A gut feeling and rare early diagnosis

Brenda and her partner, Alice.
Nearly a year later, she developed a cough. It might have been easy to dismiss. After all, coughs are common, especially when life is busy and family visits. But that timing turned out to matter. Among the relatives in town was a nurse, someone trained to notice what others might overlook. She pulled Brenda’s partner Alice aside and said plainly: “This needs to be checked.”
That moment was pivotal.
Brenda listened. She followed up. And this time, the outcome was different.
The cancer was found early, something Brenda doesn’t take lightly. Early detection gave her options, time, and the ability to approach treatment without the urgency and limitations that come with a late-stage diagnosis. She knows how rare that is in lung cancer, and she doesn’t call herself lucky casually.
Her story is a reminder that diagnosis is not always a single moment, but a series of decisions—some small, some difficult—that add up. It’s about trusting medical expertise, yes, but also trusting yourself. Brenda’s experience underscores how critical self-advocacy can be, especially when something doesn’t sit right, even if the initial answer seems reassuring.
Living fully

Beyond her diagnosis, Brenda is someone defined by far more than cancer. One of the joys woven throughout her life has always been singing. Whether performing when she was younger or sharing music in more personal settings, singing has long been part of who she is. Today, Brenda has found her way back to jazz singing, a return that feels especially meaningful. Being back in that space, reconnecting with music and performance, has brought her renewed joy and vitality. Singing is an expression of creativity, resilience, and presence, qualities that carried her through uncertainty and continue to ground her now.
Cancer has a way of narrowing focus, of making life feel smaller. Brenda’s story pushes back against that. It’s not just about what she faced, but about how she continues to live fully, with gratitude and purpose. Returning to jazz is not about going back to who she was before but embracing who she is now. She speaks openly, not because the moments leading to her diagnosis were easy, but because she hopes her experience might help someone else pause, ask another question, or seek a second opinion when something feels off.
She’s also quick to express appreciation for her doctors, for her family, and for the advocates and organizations working to change the lung cancer narrative. “Thank you to GO2 for Lung Cancer for the work you are doing,” she said. “I’m here, whatever I can do.”
Brenda’s experience is a powerful reminder that early detection saves lives, that listening to your instincts matters, and that sometimes the most important voice to hear is the quiet one telling you to look again.
GO2’s HelpLine is a free, one-on-one service that connects patients and caregivers with experienced staff who can provide guidance, resources, and, most importantly, hope. Whether it’s questions about getting a second opinion, biomarker testing, screening, treatment options, or simply needing someone to listen, the HelpLine is here to make sure you know you are not alone. Call 1-800-298-2436 or email support@go2.org to get started.

March 3, 2026

Glen lives in Hercules, CA with his Yorkie, Kuma, where he moved in 2021 to be closer to family and friends. After nearly 20 years working in the probation department, he retired at the beginning of the pandemic and began volunteering at the East Bay SPCA. What started as a way to give back quickly turned into a full-time job. These days, you’ll often find him on his daily walk to Starbucks or visiting his mom, who lives just 15 minutes away.
Jeffrey B. Velotta, MD, FACS is a thoracic surgeon at Kaiser Permanente’s Oakland Medical Center, a Clinical Professor in the Department of Clinical Science at Kaiser Permanente’s Bernard J. Tyson School of Medicine, and a clinical assistant professor in the Department of Surgery the UCSF School of Medicine. Dr. Velotta went to medical school at George Washington University. He then completed his general surgery residency at UCLA Medical Center. During this time, Dr. Velotta also completed his postdoctoral research in the Department of Cardiothoracic Surgery at Stanford University School of Medicine. Following this, he completed his training in Cardiothoracic Surgery at Brigham and Women’s Hospital and Harvard Medical School. Dr. Velotta’s clinical and research interests involve innovative techniques and regionalization pathways for all thoracic cancers and improving lung cancer screening in at-risk populations.
When Glen first noticed chest pain in the fall of 2024, lung cancer wasn’t on his radar. He was in physical therapy at the time and assumed the discomfort was muscular and temporary. But 1 test led to another, and by December, an X-ray raised concerns that couldn’t be ignored.
On December 24, 2024, Glen had a biopsy. Four days later, he received a phone call confirming cancer.
“I didn’t know what stage I was or much about what I was even being diagnosed with,” Glen recalls. “I just know it turned my world upside down.”
Glen didn’t have a smoking history, and there was no history of lung cancer in his family. Yet here he was, grappling with a diagnosis he never expected and didn’t yet fully understand.
Hearing the worst news, but not much else
Glen remembers little of the conversation that followed his diagnosis. His oncologist delivered the news with compassion, giving him permission to react however he needed.
“She said, I’m telling you the worst news I could possibly tell you. It’s okay if you get upset, scream, or cry. I’m here,” he says.
But like many patients in that moment, Glen fixated on 1 question: How long do I have to live? “I wasn’t really hearing anything else,” he says. “My best friend was with me, taking notes. I’m glad she was there because I don’t remember much of what was said. I could only think about my prognosis.”
In the days that followed, Glen did what so many people do, he went online. And almost immediately, he regretted it. “That was the worst thing I could do,” he says. “You Google stage 4 (IV) lung cancer and life expectancy, and the first article you see tells you that this is really bad news. You don’t even need to read the rest.”
Treatment, side effects, and a growing sense of fear
Glen began treatment quickly. His first regimen included radiation to his brain and chest and an infusion therapy that caused repeated breathing reactions. After 4 reactions across 2 sessions, his care team stopped the drug. He later transitioned to Tagrisso (osimertinib), which he is still on today and has tolerated much better.
But emotionally, Glen was spiraling. He describes himself as generally relatively pessimistic by nature, and the statistics he’d read didn’t help. He began quietly preparing for the end, updating legal documents, organizing passwords, and making sure his affairs were in order.
A parking lot, a 5K, and an unexpected meeting
Everything began to shift at GO2’s San Francisco 5K Walk/Run. Glen attended the event almost on a whim after finding information about it online. He arrived early, sat in his car, and debated leaving. Eventually, he got out and walked toward the event, unsure why everyone seemed so happy. “This is a cancer walk,” he remembers thinking. “Why is everyone smiling?”
A volunteer noticed he wasn’t okay and introduced him to GO2’s Senior Manager, Support Programs and Events, Michele Zeh. As Glen shared how bleak he was feeling, she pointed around the room. “This person has 10 years since their diagnosis. That person has 8,” she told him.
“And I’m thinking, how is that possible? I thought people never lived that long,” Glen says.
Then Michele asked a simple question: “Do you know Dr. Velotta?”
Glen didn’t. But meeting him was about to change his life.
“Let’s get rid of the mothership”

Dr. Jeffrey Velotta is a thoracic surgeon at Kaiser Permanente in Northern California, and one of only a small number of surgeons in the country willing to seriously consider surgery for patients with stage 4 (IV) lung cancer.
When Glen met him, the conversation felt different immediately. “He really cared,” Glen says. “I could tell right away how passionate he was about lung cancer and about the people who have it. It made me feel good.”
Dr. Velotta reviewed Glen’s scans and told him that he could be a good candidate for surgery, a treatment that might help his prognosis despite his stage 4 (IV) diagnosis. He explained his thinking using an analogy that stuck.
“We’ll get rid of the mothership,” he said.
The primary tumor, Dr. Velotta explained, was like a command center that was sending cancer cells elsewhere. If Glen’s metastatic disease was controlled with medication, removing the original tumor could still slow or stop future progression.
“The approach made sense to me,” Glen says. “You’re radiating my brain and my bones but you’re leaving where it all started? Why not get rid of that, too?”
Why surgery for stage 4 (IV) is still so controversial
Dr. Velotta is blunt about how unusual his approach still is. “I don’t think every patient with stage 4 (IV) lung cancer should have surgery,” he says. “But I absolutely believe that some should, including many more than most doctors currently consider.”
In addition to being younger, healthier, and generally fit, the key factor that makes someone a good candidate, he explains, isn’t the extent of the disease or the number of metastases, but whether disease outside the lung is controlled.
“Glen had multiple spots in his brain, bones, and elsewhere,” Dr. Velotta explains. “But his cancer was well-controlled through a tyrosine kinase inhibitor (TKI). That’s what people call ‘polymetastatic’ disease. Most surgery trials exclude patients like that. But that’s actually the majority of people with stage 4 (IV) lung cancer.”
Clinical trials, he notes, tend to focus on patients with 1 or 2 metastases, not because others can’t benefit, but because trials are designed to show clean, easily publishable results. This disconnect, he believes, is 1 of the reasons surgery remains underused for people with advanced disease. “That leaves most patients out,” he says. “And it leaves surgeons hesitant.”
A lonely position in the field
Even today, Dr. Velotta says the prevailing mindset around surgery for stage 4 (IV) lung cancer hasn’t shifted much. “The thinking is that it’s too little, too late. We’ve missed the chance to help these patients surgically. The idea is that the cat’s already out of the bag,” he says.
That assumption, that surgery can’t help once cancer has spread, is something he pushes back against constantly. “People get freaked out by polymetastatic disease,” he says. “They see multiple spots and think, ‘Oh my God, they’re everywhere.’ But if those spots are controlled, it doesn’t matter how many there are. Those patients can still benefit.”
Dr. Velotta acknowledges that his willingness to operate in these cases often puts him at odds with colleagues. “There is a stigma associated with operating on stage 4 (IV) lung cancer,” he says.
Even within his own health system, he is frequently the only surgeon willing to consider surgery for patients like Glen. “I feel very alone in this world sometimes,” he admits. “If these patients were all doing terribly, I would stop. But they’re actually doing really well.”
Instead, he says, many of his patients are living longer — and living well. “I’ve done this for 5 or 6 years. I’ve operated on many,” he says. “A lot of them are still alive. And even the ones who passed didn’t pass 3 months later. Some lived 6 plus years.”
Surgery as more than survival statistics
For Glen, surgery wasn’t just about controlling the disease. It was about reclaiming a sense of control over his own life. Surgery felt proactive to him, like taking control of his treatment and his future.
Dr. Velotta sees that psychological impact again and again. “You can’t quantify that on a spreadsheet,” he says. “But mentally, it matters a lot.”
Glen agrees. “I felt better from the moment I knew I was going to have surgery,” he says. “I can’t put that on paper, but I felt different. Better. It has helped my mindset immeasurably.”
Glen had surgery on November 12, 2025. It was minimally invasive, and he went home 2 days later. Within weeks, he was walking hills near his house. Then jogging. Then biking.
“I’m not back to where I was yet,” he says. “But I’m close. And I really don’t mind putting in the work.”
Pathology from his surgery showed just .5 millimeters of active cancer remaining in the tumor that was removed. “All I cared about was that it wasn’t inside me anymore,” Glen says.
NED — and what hope looks like now

When Dr. Velotta emailed Glen with the words “NED” or “no evidence of disease,” Glen didn’t fully grasp what it meant, but others did. “When I told people at GO2, they got really excited,” he says. “That’s when I realized, oh, this is a big deal.”
Hope, he says, is everything. “Sometimes I’m still pessimistic at heart,” he admits. “But the surgery has given me so much more reason to have hope for the future, and hope is what keeps me going.”
On sharing his story
Glen hesitated before agreeing to speak publicly about his experiences with lung cancer. Talking about cancer can still pull him into dark places. But ultimately, he agreed for 1 reason.
“If this helps 1 person,” he says. “If someone like me hears this and thinks, ‘Maybe surgery is an option for me, maybe I should ask’, then it’s worth it.”
Dr. Velotta agrees. “I just want people to know that they can ask,” he says. “That’s huge progress.”
GO2’s HelpLine is a free, one-on-one service that connects patients and caregivers with experienced staff who can provide guidance, referrals, resources, and, most importantly, hope. Whether it’s questions about biomarker testing, treatment options, or simply needing someone to listen, the HelpLine is often the first step toward feeling less alone after a lung cancer diagnosis. Call 1-800-298-2436 or email support@go2.org to get started.

February 3, 2026

When Mike Scanlon set out on a 30-day, 700-mile bike ride across Kansas, the journey ahead of him was daunting. He had 60 trails, 50 towns, and what felt like endless gravel roads ahead of him. But for Mike, who is living with stage 4 (IV) non-small cell lung cancer (NSCLC), this ride was about more than just the distance. It was about purpose and about transforming his diagnosis into something bigger.
At the heart of Mike’s journey was a principle that has guided his work and his life for years: the Athenian Oath, a commitment to leave things “not less, but greater, better, and more beautiful than they were transmitted to us.” Turning his ride into a fundraiser for GO2 for Lung Cancer and Kansas Trails Inc. was a natural extension of that belief. “I’ve always tried to live in a way that gives back,” Mike shared. “This ride felt like a way to do that — to take something personal and make it meaningful for others.”
Choosing “even if” over “only if”
Mike often described the Ride for Resilience tour as a lesson in mindset. It was one shaped deeply by his cancer diagnosis. Living with stage 4 (IV) NSCLC, he explained, can trap people in “only if” thinking: “I’ll have peace only if treatment works. Only if scans stay clear. Only if life goes back to normal.”
But the road taught him another way.
“The power of an ‘even if’ perspective is that it frees you to live with purpose no matter what happens,” Mike said. “Even if the road is uncertain. Even if outcomes aren’t guaranteed. Even if this journey reshapes your life.”
For Mike, resilience wasn’t about controlling the outcome. It was about choosing courage anyway. Pedal after pedal, day after day, that mindset carried him forward.
Trails, towns, and the strength of small places
Kansas is home to more than 4,000 miles of trails, and Mike wanted to experience as much of that diversity as possible. Riding 60 trails across 50 towns allowed him to connect not just with landscapes, but with people — especially in small, rural communities.
“I wanted to see how adaptable and resilient these towns are,” he said. “A lot of them don’t have much, but they keep showing up.”
That resilience came into sharp focus in places like Copeland, KS, population 251. A stop at the town library became a powerful reminder of shared values and of communities that quietly live out the Athenian Oath and the “even if” mentality every day. These towns, like people facing cancer, keep moving forward despite uncertainty.
Sharing the road and stories

Along the way, survivors, caregivers, and families found Mike. Sometimes it was literally on the trail, sometimes through word of mouth. They rode beside him and shared their stories.
Over the course of the ride, Mike connected with people across Kansas, creating space for honest conversations about cancer, treatment, and hope. He shared information about GO2 for Lung Cancer, including resources available to individuals and families at every stage of the disease.
“Cancer is deeply personal,” Mike reflected. “The courage it takes for people to open up always floored me.”
From a sales director at a Salina radio station to an administrative assistant at a high school in Wamego — who happened to share Mike’s same lung cancer mutation and treatment — these conversations became some of the most meaningful moments of the ride.
Hard miles and harder questions
The ride tested Mike in ways he didn’t expect, including fast farm dogs on gravel roads (most of which he could outpace, except one). But the hardest challenges weren’t physical. They were mental.
“I’ve been given an opportunity many people with NSCLC don’t get,” he said. “And I can’t waste it.”
A note from a donor, a message of encouragement, or simply the mantra JKP — Just Keep Pedaling — helped him find the answer.
The ride of a lifetime

The final day was a 93-mile ride along the Flint Hills Trail from Council Grove to Osawatomie felt symbolic. Mike saw the day as a reflection of life itself: starting early, uncertain, learning as you go, growing stronger, then feeling your body push back near the end.
And then, 2 miles from the finish, everything changed.
“I saw my grandson, Augie,” Mike said. “He wanted to ride the last 2 miles with me. And I knew his little brother PJ was waiting at the finish line with my daughter Megan.”
As Mike’s journey that day ended, his grandsons’ life journeys were just beginning, bringing the Athenian Oath full circle. “My obligation,” Mike said, “is to transmit Kansas trails — and this life — not less, but greater.”
Your turn to find your “Ride for Resilience”
Mike’s advice to anyone considering a fundraiser for GO2 for Lung Cancer is simple: define your reason.
“Mine was the Athenian Oath,” he said. “Once you know your why, invite others to help.”
Through his 700-mile journey, Mike raised more than $24,000, helping fuel GO2 for Lung Cancer’s work to increase lung cancer survival by supporting cutting-edge research, legislative advocacy, and patient support services for individuals and families nationwide.
Whether it’s a ride, a walk, a creative challenge, or something uniquely yours, your fundraiser can make a difference. As Mike’s journey shows, resilience isn’t about what happens only if everything goes right — it’s about choosing to act, even if the road ahead is uncertain.
And sometimes, all it takes is the courage to start pedaling.
Learn more about how you can create your own fundraiser for GO2 for Lung Cancer.

February 3, 2026

June & Roy live in Kennebunk, Maine, a place they moved after visiting and vacationing many times throughout their lives. They enjoy barefoot beach walks, snowshoeing, many volunteer activities focused on environmental issues, Indigenous People’s rights, social justice issues, and textile drives organized by June which have kept over 20 tons of textiles and footwear out of landfills. They also enjoy exploring Maine’s forests and mountain areas. June is a retired clinical registered dietician while Roy is a retired banking executive and director. They see a return trip to Switzerland and other excursions in their future. Their favorite toast with an adult beverage is “Ein Sache”, followed by “Uns” — German for “One Thing” and “Us”. Roy is still trying to find where June hid his heart when she stole it. She promises him that it’s in a safe place.
After a history of heart disease, Roy has learned to pay attention to his body, so when he experienced shortness of breath in July 2018, he went to the emergency room. This time, his heart wasn’t his problem. Imaging revealed a large mass in his upper right lung and, with it, a diagnosis that would reshape his years ahead.
Doctors moved quickly. A biopsy confirmed lung cancer, and additional scans showed it had spread to nearby lymph nodes, ruling out surgery. Roy was referred to David Carbone, MD, PhD at The James Comprehensive Cancer Center, where a treatment plan came together quickly.
Roy enrolled in a clinical trial led by Dr. Carbone to explore using immunotherapy in people with stage 3 (III) non-small cell lung cancer (NSCLC). He would receive immunotherapy, then radiation, then chemo, and then immunotherapy again.
The early months were manageable, and Roy didn’t experience any side effects during his initial immunotherapy infusions. Radiation and chemotherapy followed, spaced carefully over many weeks. But toward the end of treatment, a rare and severe reaction to chemotherapy landed Roy in the hospital for 10 days.
This experience forced difficult treatment decisions and required Roy to advocate for himself, something he had learned to do years earlier while caring for his late wife during her illness. Immunotherapy was paused, then ultimately stopped altogether, when Roy developed serious gastrointestinal side effects. By that point, his treatment had already achieved a complete response, and his body could not tolerate continuing.
With treatment complete, Roy entered a new phase: survivorship, including regular monitoring and cautious hope. Follow-up scans initially came every 6 months, then 9, then eventually once a year.
Judy’s story
Roy’s experience with lung cancer was not his first time navigating serious illness. Just a few years earlier, he had walked a parallel path alongside his late wife, Judy.
In November 2015, Judy collapsed in their shower at their home in southeastern Ohio. At the hospital, imaging revealed a large mass in her brain. Judy immediately understood what that meant. Her aunt had died of glioblastoma years earlier, and Judy had been one of her caregivers.
Judy underwent brain surgery the day before Thanksgiving, followed by months of treatment including clinical trials, aggressive chemotherapy, and a 2nd surgery. Despite everything, Roy remembers her determination to keep living fully and authentically, even as options narrowed.
Judy approached her illness with the same intention and creativity that defined her entire life. A spiritual director and artist, she continued creating throughout her treatment, painting, weaving, and writing as a way to make meaning of what she was experiencing. Even after a stroke affected her body’s complete left side (she was left-handed), she adapted, learning to work with her right hand and allowing her art to evolve alongside her changing body.
For Judy, creativity was not a distraction from illness, but a way of engaging with it honestly. She remained deeply connected to people around her and committed to living as fully as possible, even as she faced her reality of a terminal diagnosis.
“She always showed us how to live,” Roy recalls a close friend saying about Judy. “Now she’s showing us how to die.”
Keeping a promise
Judy died in October 2016, after time in hospice that Roy describes as both heartbreaking and deeply meaningful. In his following years, he turned to journaling as a way to survive his abysmal grief.
“For 2 years, I journaled every day,” Roy said. “Sometimes 2 or 3 times a day, whether I was on my porch or in a local pub or a restaurant or the Grand Canyon, you would find me with my journal in hand.”
His writing became a form of self-therapy, a place to hold and process anger, memories, gratitude, and loss all at once. Over time, it also became the foundation for something Judy had asked Roy to do before she died.
“She made me promise to publish her art and her words,” Roy said. “And I said yes, not knowing at the time what that might look like.”
The result was a book built from Judy’s artwork and writing and interwoven with Roy’s journals to become a 3-part story about living well, dying honestly, and finding a way forward. What began as a promise became a project that took 5 years to complete and eventually reached far beyond Roy’s immediate circle. They edited over 950,000 words from him and Judy down to about 85,000 for the book.
Roy is clear that their memoir and award-winning love story was never meant for a narrow audience. It has resonated with people navigating serious illness, caregivers walking alongside loved ones, and healthcare professionals seeking to better understand the lived experience of patients and families.
“I’ve heard from hospice workers, nurses, and social workers who said it helped them better understand the people they care for,” said Roy. Others have told him they read the book not because they were facing illness themselves, but because they wanted to understand who they hoped to be when life becomes difficult for them.
Today, Roy and his new wife, June, give the book, “It All Belongs,” away freely, believing it is meant to be in people’s hands rather than on a warehouse shelf. Copies are available at no cost, with readers asked only to cover shipping. To learn more or request a copy, visit http://itallbelongsbook.com and use code “GO2Cancer” for your free copy.
June
June had been part of Roy’s life long before his lung cancer diagnosis. June met Roy’s late wife Judy through their Ohio church and became close friends. After she died, June and Roy became support for each other, and when Roy learned he had lung cancer, June was one of the first people he called.
“She screamed,” Roy remembered. “And I hated making her feel such pain.”
At that time, June and Roy were just beginning to recognize their growing feelings for each other, but for June, her decision to stay, to support Roy, and eventually to build a life together was instinctive.
“I had this voice that said, ‘I’m not going to let him go through this by himself. He’s already lost his wife of almost 40 years and had more than enough pain from her death,” she said. “I didn’t care where we were going to go or what we had to go through. I was in.”
When Roy proposed, he made sure June understood the reality of his diagnosis. “I said, ‘Do you realize I may not be here in 2 years?” he recalled.
Her answer was immediate. “Well, it’ll be the 2 best years of my life.”
June attended every appointment and every treatment with Roy, and their love deepened even as they navigated all of lung cancer’s difficult challenges together.
They married in Iona, Scotland during Roy’s treatment, after asking his care team whether it was safe to travel. Their answer was yes, and the moment became one of joy woven into a difficult chapter.
What comes next
For more than 5 years after completing treatment, Roy’s scans remained clear. Then, in the fall of 2025 during a routine follow-up appointment with his new oncologist at the Dana-Farber Cancer Institute after a move to Maine, everything shifted again.
“Dr. Sands walked in,” Roy said. “And for the first time he didn’t say, ‘We didn’t find anything.’ Immediately, I knew something was wrong.”
A new tumor had appeared in the same area of his lung that had already been heavily treated. Because of prior radiation and scarring, many treatment options were no longer possible.
“Every option we brought up – radiation, surgery – they just kept getting pushed off the table,” Roy said. “That has been really hard.”
After consultations with multiple specialists, Roy and his care team determined that immunotherapy would likely be their next step. They are currently waiting on additional testing to confirm this as their treatment course, and Roy is eager to get started. While their next steps are currently uncertain, Roy is not without perspective.
“For me to be loved by two such incredible women and to be able to love two incredible women in one lifetime,” he said, “I don’t need a whole lot else. We’ll figure out the rest.”
If you or a loved one are facing similar uncertainty—whether newly diagnosed or navigating what’s next—GO2’s LungMATCH team can help you understand treatment options, including clinical trials, and talk through next steps. Call 1-800-298-2436 or email support@go2.org to connect with a LungMATCH Navigator. to connect with a LungMATCH Navigator.

January 5, 2026
Robyn and Bob Washburn live in Simi Valley, CA where they like to spend time with family, enjoy the outdoors walking and taking hikes when they can, and go on adventures with their Corgi, Teeter Moosie. Robyn has worked as a Senior Paralegal for over 35 years at The Burbank Firm, L.C. in Burbank, CA, and Bob is a retired advertising executive in the fitness industry who now enjoys day-trading. They are looking forward to good health, more traveling adventures, and numerous grandchildren! Their mantra is: “Make each day count, living life one breath at a time.”
When Bob and Robyn Washburn talk about the last 4 years, they describe it as a story that’s “a little bit like the Griswolds,” with 1 challenge after another, and moments so unbelievable they can only laugh at it all. But beneath the events that have seemed chaotic and even devastating at times is something much simpler and more powerful: a partnership built on deep love, determination, and the unshakeable belief that there is always a path forward, together.
For the Washburns, “together” has guided their experience. From the accident that revealed a hidden lung nodule, to months of long-COVID leading to heart failure, to a stunning set of medical missteps that delayed Bob’s diagnosis for more than a year, their story is marked by frustration and heartbreak, but also resilience, community, and a renewed capacity to hope.
A car accident, COVID-19, and a missed warning sign
Bob’s path to a diagnosis began with an accident that had nothing to do with cancer.
In June 2020, he was hit head-on by another driver and rushed to the emergency room. Imaging revealed a small lung nodule, but doctors reassured them that it wasn’t alarming. “A nodule meant nothing to us,” Bob recalls. “It wasn’t red alert. We were told time and again that it was nothing to be concerned with.”
With no clear reason to worry, they went home, focused on healing from the crash.
But within a couple months of the accident, both Bob and Robyn became sick with COVID and remained sick for months as it developed into long COVID. Bob developed serious breathing issues followed by congestive heart failure. Their lives narrowed to managing day-to-day symptoms, seeking answers from specialists, and trying to understand what was happening to Bob’s heart and lungs.
“We were down for months,” Robyn says. “At times, Bobby couldn’t speak. He really needed to be hospitalized, but they wouldn’t take him.”
Amid the chaos of long-COVID and the overwhelmed healthcare system of late 2020, the original lung nodule that had been identified in the car accident faded into the background. Though the nodule appeared again on imaging ordered by Bob’s cardiologist, no one explained that it could be serious. There were no urgent referrals and no clear next steps.
“It was COVID times,” Bob says. “Everyone was distracted.”
“No one ever said, ‘We think this could be cancer,’” Robyn says. “They only ever said, ‘We’ll watch it.’”
Nine months of waiting and a diagnosis delivered by accident
By early 2021, as Bob’s heart function gradually improved, the Washburns finally had the capacity to revisit the unexplained nodule. They pushed for appointments with a pulmonologist, hoping to get clear answers. Instead, they faced continued delays and uncertainty.
Months passed with vague reassurances and no urgent action. Robyn remembers feeling powerless and furious.“It was a comedy of errors, but not funny at all. We waited another 9 months. We didn’t have the capacity at the time to say, ‘We’re not satisfied,’ because we were drowning.”
Finally, in September 2021, 15 months after the nodule was first discovered, Bob underwent a biopsy. But even then, they didn’t receive the results from a doctor. Instead, a lab employee, calling solely to request consent for biomarker testing, casually told Robyn the words no one should hear from a stranger: “You need to sign a consent because your husband has cancer.”
“I just about lost it at my desk,” she remembers. “Now I had to be the one to tell my husband he had lung cancer. It wasn’t a doctor explaining anything; it was a lab worker checking her list.”
When they finally met with the pulmonologist in person, the physician was visibly shaken. “He was sweating,” Bob recalls. “He knew he’d made a huge oversight.”
Finding answers and the right path forward
Once Bob actually received his diagnosis, the couple quickly had to consider treatment. Bob’s biomarker testing showed an ALK rearrangement, a type of mutation often highly responsive to targeted therapy.
They were introduced to the possibility of clinical trials, surgery, and targeted therapy all at once, while still trying to catch their breath from the shock of the diagnosis.
“We came in not knowing anything,” Bob says. “And suddenly we had to learn everything.”
Initially, doctors explored whether the tumor could be surgically removed. But new imaging revealed the cancer had spread to the other lung, and then, in what felt like one more blow, to the spine, making him stage 4 (IV). Each new scan shifted the treatment plan, narrowing options and adding urgency.
There were many moments that felt surreal. For a time, Bob was being considered for a clinical trial, and the couple spent weeks working with the trial team to qualify and complete required testing. During a call about that trial, a doctor casually chatted about the artwork behind them on Zoom before abruptly telling them that Bob was no longer eligible. “We spent so much time with him, and then we never heard from him again,” Bob says.
Breathing again
Bob began taking alectinib in November 2021, about 2 months after his biopsy. By then, he was struggling just to walk up a flight of stairs.
“I could feel it; I was declining,” he says. “It was scary. I knew something was really wrong. I was dying, essentially.”
Within weeks of starting targeted therapy, he felt a shift. His breathing eased. His energy returned. The first post-treatment scan confirmed what he already sensed: the medication was working.
“That first scan showed progress,” Bob says. “And more importantly, I could feel there was progress in my body.”
More scans brought more good news. The spot on his spine disappeared and the cancer in his lungs shrank. Over time, he stabilized fully.
“I’m basically NED right now,” he says. “Nothing on my spine. Just a little residual, and that’s okay.”
Four years later, Bob remains on alectinib with excellent results. They continue scans every 3 months, and with each clean result, their world opens a little wider.
Finding the right team and a community that feels like family
After the difficult start to their diagnostic experience, the Washburns made a change in their care. They transferred to City of Hope and found oncologist Dr. Ravi Salgia, whose expertise in ALK-positive lung cancer, and his personal kindness, made an immediate difference.
“He’s just fabulous,” Robyn says. “We know he truly cares. He was the right fit for us.”
Remarkably, they first met him not in a clinic, but at the GO2 SoCal 5K Walk/Run. From there, their involvement with the lung cancer community deepened. They have since attended ALK Summits, watched Lung Cancer Living Room® sessions, participated in local walks, and gotten to know other families navigating similar paths.
“We follow so many stories now,” Bob says. “We pray for these people. When we see them at events, we’re hugging each other like family.”
Moving forward and finding joy again
As Bob regained strength, the couple began reclaiming parts of their life that had been on hold. They’ve traveled to Texas 3 times in the past year to see their daughter graduate with her doctorate in physical therapy, see their granddaughter be born, and spend her first Christmas together. Another milestone took them to Idaho, where Bob had the joy of walking his daughter down the aisle at her wedding. Another daughter, Brooke, has been a great support to them, including participating with them in GO2 5K Walks. They’ve also jumped into new opportunities, including Bob’s role as a Genentech ambassador, where he shares his story to help others.
“You wouldn’t believe the things he does now,” Robyn laughs. “Talking to people, getting out there; it’s amazing.”
Bob smiles. “I’m a private person. At first, I didn’t want anyone to know about my diagnosis. I didn’t want, ‘Poor Bobby.’ I isolated myself. But that wasn’t the right way.”
Now, the opposite is true. Their world is bigger, their community wider, and their bond—already strong—has deepened. Through it all, their love story has been its own anchor.
When asked what Robyn has meant to him through this experience, Bob’s voice softens: “She’s my eyes, my ears, my brain. She figures things out when I say forget it. She’s a dog with a bone, in a good way,” he says, smiling. “She made me a better person, and I wouldn’t be here if she wasn’t here.”
Robyn laughs. “And he takes care of me too. We’re a great team. We’ve been through everything together. We’re 100 percent connected.”
Their partnership shows up in small ways too, like the matching outfits Bob now wears willingly to every appointment.
“If you really knew me,” he says, “you’d say there’s no way I would do that, but here I am.”
“He even picks out the shirts now,” Robyn adds.
Reclaiming hope
For Bob, hope isn’t an abstract concept. It’s deeply practical.
“I’m a glass-half-full person,” he says. “Hope, for me, is a vision. It’s imagining us traveling more and watching our family grow.”
Robyn adds, “There was a time we didn’t know if we could do anything. We were stuck. Now we have things to look forward to, and that gives us hope.”
Their faith plays a role too.
“We’re trying to normalize something that’s been very abnormal,” Bob says. “But we don’t take anything for granted. We know how blessed we are, and we give thanks for that.”
Advice for others hearing the words: “You have lung cancer.”
When asked what they would tell someone newly diagnosed, Bob doesn’t hesitate.
“Take a deep breath,” he says. “Know that there are solutions. Lean on doctors, support groups, and organizations like GO2. Reach out. You will not embarrass yourself. You will not be judged. It’s overwhelming, but you’re not alone.”
Robyn jumps in gently: “And rely on your care partner to listen for you. That’s what’s hardest. People isolate themselves. They don’t want to talk. But listening, sharing, getting support, it can change everything.”
Bob nods. “I wasted 6, 7, 8 months isolating myself. If I can help anyone, I’d say, get out there and get yourself uncomfortable. People really do care.”
GO2’s HelpLine is a free, one-on-one service that connects patients and caregivers with experienced staff who can provide guidance, resources, and, most importantly, hope. Whether it’s questions about biomarker testing, treatment options, or simply needing someone to listen, the HelpLine is often the first step toward feeling less alone after a lung cancer diagnosis. Call 1-800-298-2436 or email support@go2.org to get started.